

“In this room, they can perform a C-section if they think it necessary”, explained Luísa Pinto, Obstetrician at the Santa Maria Hospital and trainer of the Training Course in Obstetric Emergencies. In the large room that recreates a delivery room, Lucina the simulation mannequin is ready to be used to practice the resolution of various emergency situations, including concrete obstetric maneuvers.
While giving the guided tour to a group of 6 doctors (internists or specialists in Obstetrics and Gynaecology) and 6 nurses (only one male nurse) specialized in maternal and obstetric health (ESMO), Obstetricians Luísa and Mónica Centeno organized the group in two teams. Accompanying them, three ESMO nurses from the Hospital stressed some information and listed all the materials and drugs available to be used in the practical workshop.
Each team, composed of 3 Obstetrics and Gynaecology interns or specialists, 2 ESMO nurses and an Anaesthesiologist, were to be subjected to six emergency situations, testing their reaction to pressure, their ability to communicate with the team, the patient and family members, reinforcing leadership techniques and team performance, as well as their ability to solve situations that are exceptionally rare in daily life. However, and because these situations are not impossible to occur, and despite those teams are already residents, more experienced in Obstetrics, what would they be able to respond without much time to organize their thoughts and if they barely knew the rest of the team? How would they react without a complete medical record and time to plan the best medical action?
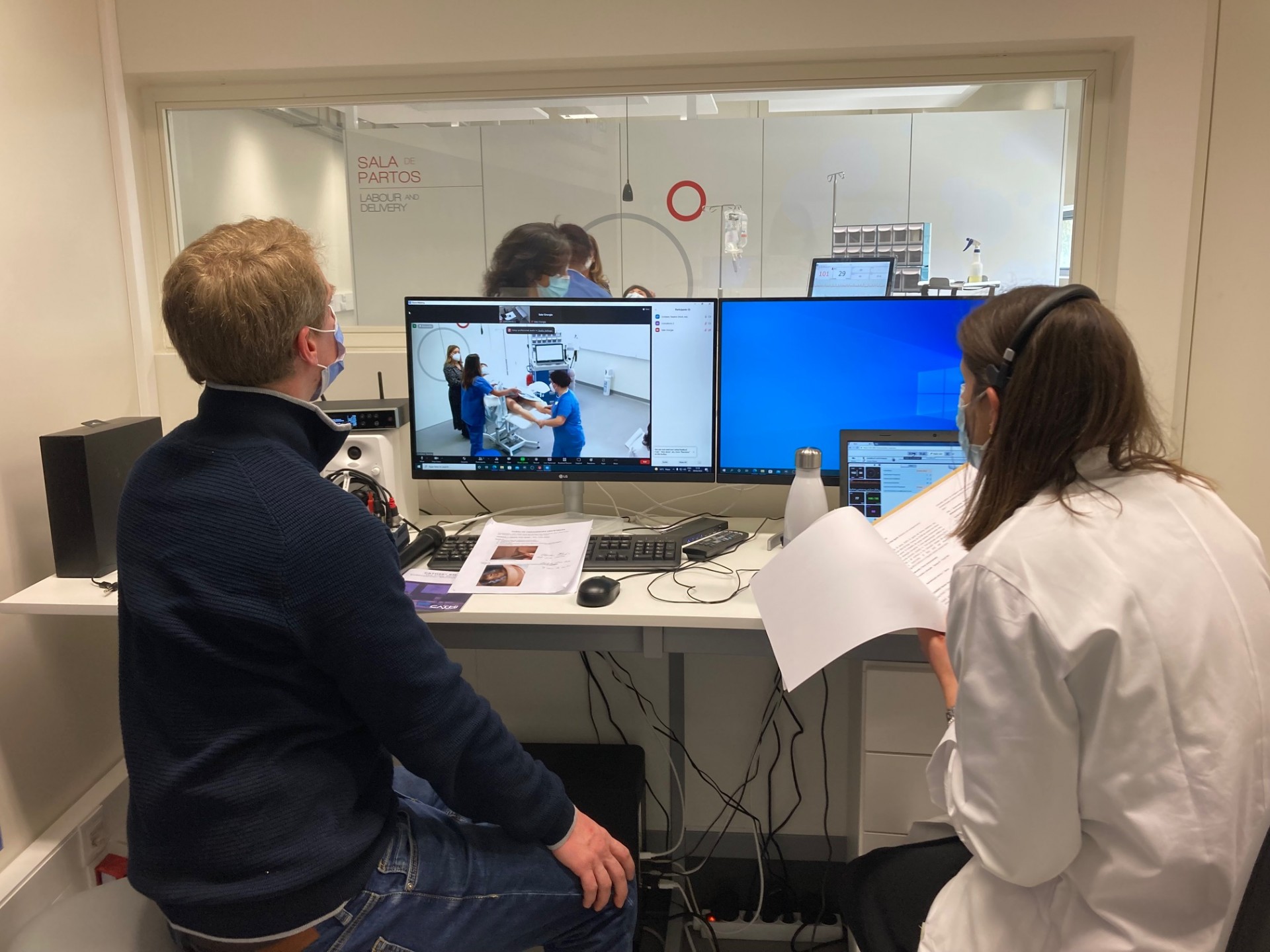
In the moment between the preparation of the control room, which had two actresses/interns, an engineer (the indispensable Cristiano Tavares) and a doctor who was preparing the model for the next scene, you could feel a certain tension in the air. If it were to be simple, maybe none of those elements would need to be there. But when it's the first time that a doctor or nurse is faced with acute situations that require an effective reaction in a matter of minutes, where does one get the knowledge to take action?

At what point in one’s career does one train for the big clashes before they happen in reality, with real patients and babies?
There have been many approaches to the evaluation of clinical teams, even while they are only students. In an increasingly accelerated Medicine practice in the global world and with the imposition of advanced technology, how effectively would professionals prepare themselves for the present times? Will there be time for experience to guide those just starting out on their path?
In response to the pressing needs of those whose professions involve human lives, a vast technological simulation space was implemented that allows to reliably recreate extreme clinical situations, in limited time.
Time was precisely the first element to be met with no margin for error. At 1 p.m. sharp Luísa Pinto was waiting in the operating room for the entire team to finish getting into their blue operating room suits. Mónica Centeno was speeding up the slight delays of those arriving from other hospital units and wanted to meet the time with the same precision.
First case. One team in the block. The other team gathered in a conference room and watched in silence. Acute fetal hypoxia – the fetus had a marked and prolonged drop in heart rate. Not being previously presented with the patient's condition, no one could predict what was coming, because acute fetal hypoxia was not announced. Only the mother's vital signs, the fetal heart rate, and the voice coming out of the simulator, controlled by a real person in the control room, hinted that something serious was going on. If team action was not taken within a few minutes, the probability of very serious injuries to the baby, or even death, could happen. This was enough to later understand why was so vital to respect time, since reacting within 3 to 5 minutes would be more effective than in 12, and after 15 minutes it would be possibly a fatal scenario.
Hastiness was an equally strong element, since an impulsive decision due to time pressure could be just as reckless as a lack of reaction. Once the exercise was over, the two teams gathered in the room to analyse the case. As self-evaluations were asked for, the team that was observing was asked to reflect on their observations. With no competition, and no attempt to have leading roles, or winners, even though it was a fictitious scenario, for no moment did it feel that they couldn’t take it seriously.


Two performances for each case. Two teams would take turns testing behaviours, actions, and techniques. With each exercise, the individual behaviour would turn into group behaviour, and the most individual action would take on a newly won team spirit. Throughout the action the trainers thoroughly observed the words and gestures, without any interference or words. "We are here, but forget we exist, don't ask anything because we won't answer".
More scenarios followed. Cardiopulmonary arrest. Retention of the after-coming head. Postpartum hemorrhage.
In the interaction between real teams, simulator and medical actresses, approaches changed. Anxious family members intervened, pregnant women panicked, teams learned to stop communicating separately and become a real team with active communication. In the control room, the sound of a woman filled with pain and fear increased the realism that became an indispensable element for those who live the decision running against time. At each scenario, new evaluation among all and new dynamics. New actions to improve. Better conclusions.


Each debriefing between teams allowed the room and the simulator to be prepared again for the next test. Always with medical help, Engineer Cristiano adjusted his technique piece by piece, fitting each one in its precise place. That is to say, he already knew where to place the placenta and the baby in position for birth.
In the control room, people spoke only if they had to, and on the action stage people moved as if in a silent waltz that needed to move towards the same side so as not to break the choreography. The noise of time passed loudly for those who were spectators in the control room, but it flew by for those who wanted to solve the situations and searched in apparent calm for the right answer.
Leadership in emergency situations was discussed. Communication and feedback. Always the truth, even to those at risk, even if it was a limited data kind of truth, but always the truth. New scenario. New team. New assessment.
Change of set. This time the delivery room was resting. It waited for a new story. We go to the doctor's office. New silence for those not in action. The same pressure that didn't allow any tiredness to settle among the teams and the examiners.
After a whole afternoon of adrenaline-pumping situations, the end of the afternoon came with the end of the scenarios and a unanimous feedback of mission accomplished and strengthened learning. Some had been waiting for some time for the right opportunity for this training, they showed that it was worth the waiting and the group guaranteed a return to refine new and more techniques.

Who is behind the project?
With a PhD in Obstetrics in 2021 from the Lisbon Academic Medical Centre (CAML), with a thesis entitled "External Cephalic Version: Impact of simulator training and communication skills training", Luísa Pinto Grilo has been an Obstetrician for 26 years.
Always with grades reaching the maximum scale of merit, Luísa got into the Faculty of Medicine of the University of Lisbon in 1984. This was followed by a Masters in "Adolescent Health" (2011 / 2015) and a Post-Graduation in "Specialization in Introduction to Clinical Research: practical course" (2017 / 2018). In the 6th year of Medical School and at the beginning of the 2nd year of the General Internship, she worked in clinical research as a scholarship holder of the National Institute for Scientific Research (INIC), in the area of movement disorders, specifically in the use of botulinum toxin in situations of dystonia.
As a result of this work, guided by Professors Castro Caldas and Cristina Sampaio, she is now co-author of several publications and scientific papers in this area, nationally and internationally. Member of the Technical Committee for the Certification of Medical Termination of Pregnancy and president of the same committee since 2019, she is also a jury of exams for equivalence to the specialty of Obstetrics and Gynaecology. Luísa Grilo is invited assistant of Obstetrics and Gynaecology at FMUL, responsible for the theoretical, theoretical-practical and practical classes of the 5th year and she guides the 6th year in their clinical internships in Obstetrics.
In 2012 she created the Nephro-Obstetrics consultation and established new connections with various specialties (cardiology, hematology, psychiatry, urology, gastroenterology), in order to provide support to the pregnant women she received in her consultations. She coordinated the ER as well as the Preconception Consultation. Working mainly in the field of Maternal-Fetal Medicine, since 2021, she has been a subspecialist in this area. She is currently the Director of the Obstetrics Department at the North Lisbon University Hospital Centre (CHULN), by delegation of functions.
So we decided to find out more about the preparation of the cases and the expertise of the Obstetricians who prepare the simulation cases, how real classes are prepared for experienced professionals, and what Medicine and its teaching have to offer with this new training technique.


Since when did these trainings with simulators recreating reality start?
Luísa Pinto: At the CHULN we started to hold training courses in Obstetric Emergencies in June 2017, initially at the Obstetrics Department facilities and with models with less potential. Since 2021 we have been using the Simulation Center facilities in the Reynaldo dos Santos Building and a more modern model with more possibilities in terms of training in obstetric and other situations.
How were the 6 clinical cases presented in this training designed and planned?
Luísa Pinto: The 6 scenarios we trained correspond to the main emergency situations in obstetrics.
How was the transition from theory to practice done until now? In the field and with real patients?
Luísa Pinto: Simulation courses in obstetric emergencies have existed for several decades in other countries and later emerged in other hospitals in the country, so it was possible to do the training in these centres. We currently have a centre with excellent conditions in terms of facilities and simulator, which allows us to conduct this course with a high level of quality, integrating multidisciplinary teams (obstetricians, anesthesiologists, and nurses) and promoting not only gesture training and clinical performance but also training in communication (within the team, with the pregnant woman, and with the accompanying person) in emergency situations, a fundamental aspect for the success of interventions.
Despite the amount of experience and training one has, can a new case arise that changes the perspective of a clinical case?
Luísa Pinto: In Medicine different and unique situations can always arise, since no two people are alike and each reacts in their own way. In any case, there is a pattern of action common to the various situations that, if trained regularly, allows the resolution of most situations. This training is particularly important in scenarios which, due to their rarity, do not allow for regular practice in the real context, however, due to their severity, can make a total difference in the obtained outcomes.

Joana Sousa (contents)
Leonel Gomes (photo report)
Editoral Team